

What if hot flashes and night sweats weren't random? What if something measurable in your body, years before your final period, could influence when they'd start and how long they'd last?
A new study published in the Journal of Clinical Endocrinology & Metabolism suggests that fasting insulin levels in your late 40s may do exactly that.
This matters because insulin is modifiable. It responds to lifestyle changes, often before your weight changes. Which means you're not waiting for symptoms to arrive. You have a lever you can pull.
What the study found
Researchers followed 704 women for over 10 years through the Study of Women's Health Across the Nation (SWAN). They measured fasting insulin levels at age 47 and tracked when women first experienced vasomotor symptoms: hot flashes, night sweats, and cold sweats.
The findings were clear. Higher insulin levels at age 47 were associated with younger onset of hot flashes and night sweats. They were also associated with longer duration of hot flashes and cold sweats.
But the headline finding is this. When researchers looked at insulin, BMI, and fasting glucose together in the same model, only insulin showed a significant independent association with hot flash incidence. BMI didn't reach significance. Glucose didn't either.
That's unusual. We've spent years hearing that body weight drives menopausal symptoms. This study suggests insulin may be the more direct player when it comes to hot flashes.
Why insulin, not just BMI?
Insulin and BMI affect different aspects of the menopausal transition.
In this study, BMI at age 47 was significantly associated with oestrogen decline and FSH dynamics across menopause. But it wasn't linked to testosterone changes. Insulin, on the other hand, was significantly associated with a steeper rise in testosterone, but not with oestrogen or FSH trajectories.
So both matter, but they seem to influence different biological pathways. And when it comes to hot flashes, insulin appears to be the more sensitive marker.
The metabolic thread running through this
Your metabolic health doesn't sit in the background. It connects your energy, your hormones, and how you experience menopause.
Insulin is a metabolic signal. When it's consistently elevated, it reflects how your body is managing glucose, inflammation, and energy regulation. And those processes may influence symptom timing and duration.
The important bit is that insulin levels can be elevated before you develop clinical insulin resistance. Emerging evidence suggests this can happen before weight gain, before fasting glucose rises, and before HbA1c flags a problem.
Which means waiting for those other markers may miss a window where small changes could make a meaningful difference.
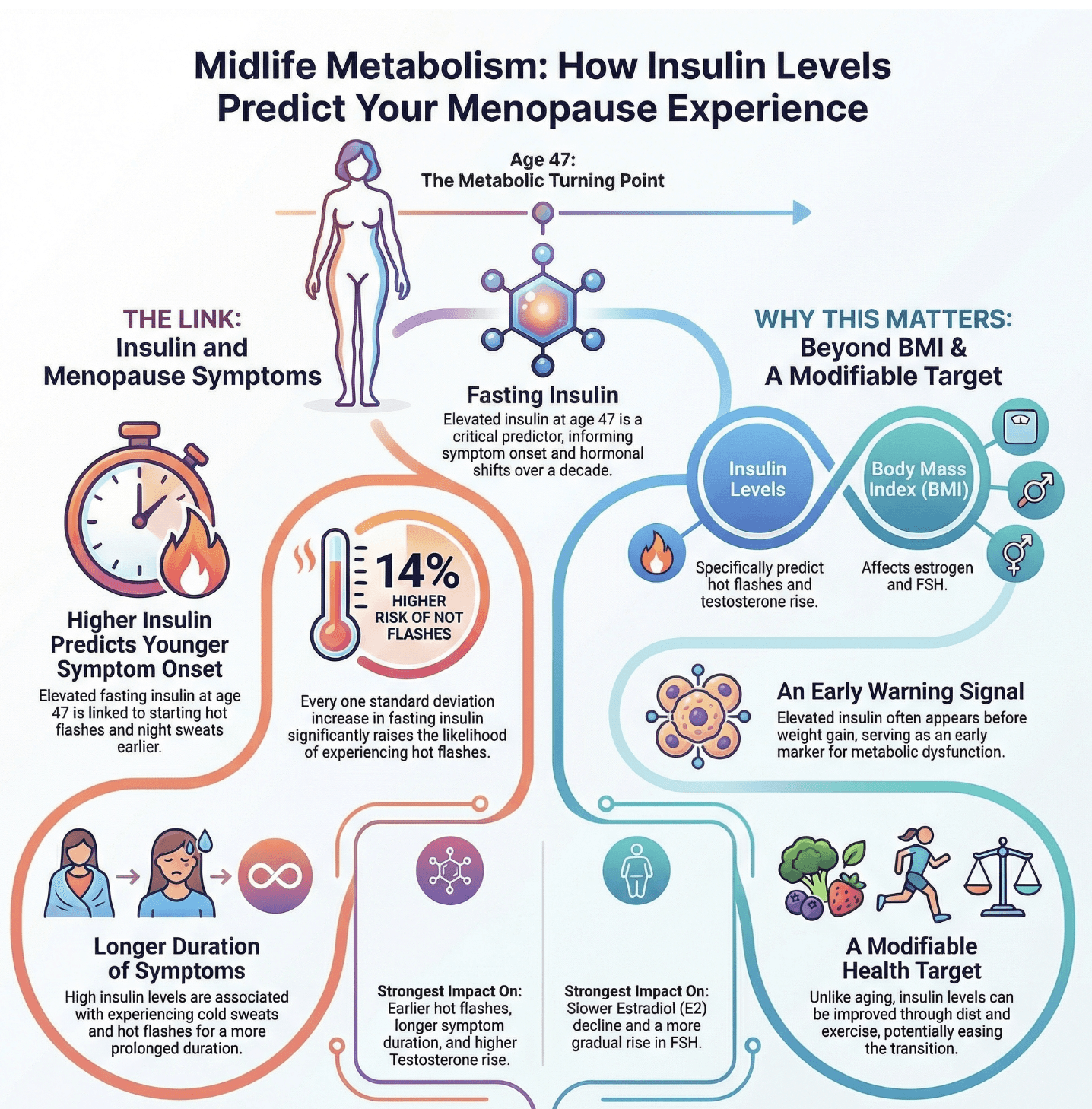
Key findings from Athar et al. (2026): how insulin levels in perimenopause relate to menopause symptoms.
What I see in clinic
Hot flashes and night sweats are disruptive. But they're often not the only thing happening.
In my clinical practice, I regularly see women in their late 30s and 40s describing brain fog, joint pain, low energy, and heightened anxiety, (often alongside many other symptoms). These symptoms aren't measured in this particular study, but broader metabolic research supports the link between glucose instability and each of these experiences.
When insulin is chronically elevated, blood sugar regulation becomes less stable. That volatility can show up as energy crashes, difficulty concentrating, and mood shifts. It also contributes to systemic inflammation, which is linked to joint discomfort and pain.
So yes, this study focuses on vasomotor symptoms. But the metabolic patterns it identifies have wider reach.
Why this gives us a lever to pull
Here's the hopeful part. Insulin responds to lifestyle interventions. Evidence from exercise research suggests that aerobic and resistance training can lower insulin levels and improve insulin sensitivity, independent of weight loss.
That's not the same as saying exercise prevents hot flashes. This was an observational study, so we can't prove causation. But it points us toward something actionable. If higher insulin in perimenopause is associated with earlier and longer-lasting symptoms, and if insulin is modifiable, we have a direction to move in. Alongside exercise, we can find practical powerful action points based on nutrition, circadian rhythm, sleep and stress management all of which can support lower insulin levels and improved insulin sensitivity.

It's also worth noting that age 47 was chosen as the measurement point for practical reasons, not because it's a biological turning point. The average age of final menstrual period in this study was 51. So for most women, insulin levels at 47 reflect mid-to-late perimenopause. That's still a window where intervention is possible.
What you can do
You may not have access to fasting insulin testing. It's not a marker GP practices routinely use. But you can look at proxy indicators of insulin sensitivity.
Signs that insulin may be elevated:
Waist circumference above 80 cm (for most women), elevated triglycerides and low HDL cholesterol (a high triglycerides-to-HDL ratio is a useful marker), blood pressure creeping upward, fasting glucose in the upper end of normal range (above 5.6 mmol/L).
If several of those are present, consider the steps below which can help you improve how your body responds to insulin.
Practical steps to support insulin sensitivity:
Start with one. You don't need to overhaul everything at once.
Add resistance exercise. Bodyweight squats, press-ups against a worktop, resistance bands. Two or three times a week. Muscle is metabolically active tissue, and building it improves insulin sensitivity.
Walk daily. Consistent, moderate-intensity movement helps regulate blood sugar. Starting with just 5 or 10 minutes is a great way to build the habit. For the best results, try to do it right after meals.
Support your circadian rhythm. Get bright light exposure in the morning (even on overcast days). Dim lights in the evening. Sleep and wake at consistent times. Your metabolic system runs on a 24-hour clock, and disrupting it affects insulin regulation.
Stabilise your meals. Include protein with every meal. Reduce refined carbohydrates (white bread, pastries, sugary snacks). Find meals and snacks you love which keep your blood sugar steady. This prevents blood sugar spikes, so your body doesn't have to pump out extra insulin to bring your levels back to normal.
If you're already doing some of these, brilliant. If not, pick the easiest one and try it for a week. Notice what changes.
What this study doesn't tell us
This is one observational study. It can't prove that lowering insulin will reduce vasomotor symptoms. It shows an association, not causation.
Age 47 may not represent the same stage in every woman's menopausal transition. Some women will be earlier in perimenopause, others later. Individual variation is real.
And vasomotor symptoms are multifactorial. Genetics, stress, sleep quality, other metabolic factors, and hormonal patterns all play a role. Insulin is part of the picture, not the whole picture.
But it's a part we can measure and influence. That's what makes it useful.
The takeaway
Higher insulin levels in your late 40s may be associated with earlier onset and longer duration of hot flashes and cold sweats. That association held even when researchers accounted for BMI and fasting glucose.
Insulin is modifiable. It responds to movement, sleep, circadian rhythm support, and dietary patterns. Often before your weight changes.
So if you're in perimenopause, or approaching it, this is something you can assess and act on now. Not to guarantee symptom-free menopause, but to give yourself the best metabolic foundation for whatever lies ahead.

If you want a structured approach to assessing your metabolic health and building a roadmap tailored to your symptoms and goals, that's what I do. You can find out more about working with me [here].
Start with the easiest lever this week.
References
Athar F, Gregory S, Houston EJ, Templeman NM. Insulin Levels Early in Perimenopause Inform Vasomotor Symptom Incidence Across the Menopausal Transition. J Clin Endocrinol Metab. 2026. DOI: 10.1210/clinem/dgaf699.
